Wednesday, 18 August 2021
Friday, 23 July 2021
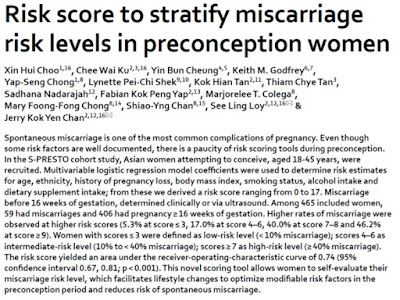
Miscarriage Risk Score
Found this research article written by KKH doctors (and my IVF doctor is part of the team).
(Click on image to go to website.)
My paraphrase of the formula from the article:
Add up the score of the factors that applies to you.
Of course, I am interested to find out what's my risk score. Based on the formula, my score is 6, translating to intermediate risk of 17%, which doesn't seem too bad. However, the sample size of "age 35 and above" is only 37 (8%), which is probably not large enough.
In case you are not familiar with scientific research methodolody, I want to mention that every research has its limitations, which are often mentioned in the article itself. Hence, to get the full picture, you need to read this part too.
(Click on image to go to website.)
My paraphrase of the formula from the article:
| Miscarriage Risk Factors | Scores |
| Age 30 to 34 | 2 |
| Age 35 and above | 4 |
| Indian | 2 |
| History of pregnancy loss | 2 |
| Underweight (BMI below 18.5) | 2 |
| Overweight (BMI 23 and above) | 1 |
| Smoker | 3 |
| Alcohol intake above 250 ml/week | 2 |
| No dietary supplement intake | 2 |
Of course, I am interested to find out what's my risk score. Based on the formula, my score is 6, translating to intermediate risk of 17%, which doesn't seem too bad. However, the sample size of "age 35 and above" is only 37 (8%), which is probably not large enough.
In case you are not familiar with scientific research methodolody, I want to mention that every research has its limitations, which are often mentioned in the article itself. Hence, to get the full picture, you need to read this part too.
Monday, 12 July 2021
Blastocyst Pendant

(Click on image to go to Instagram.)
I have a photo of my mini J when he was still a blob of cells. Not all mothers have the privilege to own such a photo.
Thursday, 8 July 2021
My Story on Fertility Support SG

(Click on image to go to Instagram.)
Thanks for the opportunity to share my story.
Wednesday, 2 June 2021
IVF Fresh #3 Summary
Pre-Cycle Counting Down
IVF Fresh Cycle 3
Comparing my three fresh cycles
| 2 months | Consultation with Dr Sadhana Blood test to measure my AMH HIV blood test for hubby because his has expired |
| 7 weeks | Pelvis ultrasound at Thomson Medical Centre (to skip long queue at KKH) |
| 6 weeks | Hubby went for sperm analysis |
| 3 weeks | IVF Briefing / Counselling |
IVF Fresh Cycle 3
| CD1 | Call KKIVF |
| CD2 / Stim Day 1 | Baseline scan: small follicles in both ovaries; lining 5 mm 350 IU Gonal-F injections daily for 4 days |
| CD6 / Stim Day 5 | 350 IU Gonal-F & 0.25 mg orgalutran injections daily for 2 days |
| CD8 / Stim Day 7 | Largest follicle at 14 mm 350 IU Gonal-F & 0.25 mg orgalutran injections daily for 3 days |
| CD11 / Stim Day 10 | Largest follicle at 20.5 mm 350 IU Gonal-F & 0.25 mg orgalutran injections daily for 1 day |
| CD12 / Stim Day 11 | Largest follicle at 23 mm Last 0.25 mg orgalutran injection in the morning Trigger injection (triptorelin) at 9.30 pm |
| CD14 | ER at 9.30 am (reporting time 8.15 am) |
Comparing my three fresh cycles
| Fresh #1 Dec 2015 | Fresh #2 Feb/Mar 2017 | Fresh #3 May 2021 | |
| AMH | 7.4 ng/mL | - | 4.7 ng/mL |
| FSH injection | 300 IU Puregon | 250 IU Puregon | 350 IU Gonal-F |
| No. of eggs retrieved | 24 | 30 | 16 |
| No. of embryo frozen | 6 Day-2 | 5 Day-5 | 1 Day-5 |
Wednesday, 5 May 2021
PGD becomes Mainstream Clinical Service
Here's a good news for those seeking PGD at private clinic/ hospitals. I don't see any significant difference for those at public hospitals, but I'm definitely not the best person to comment on this since I have not gone through it myself.

(Click on image to go to website.)
(Click on image to go to website.)
Thursday, 4 March 2021
PGS Statistics
Who is eligible for PGS trial?
[0:25] (1) 35 years old and above, (2) suffered 2 or more recurrent implantation failures, or (3) experience 2 or more pregnancy losses
How much does it cost the government?
[1:07] $1.7 million
How much does it cost the patient?
[1:23] $1,100 per test on average for consumables + $2,500 to $4,500 for embryo biopsy
What is the success rate?
[1:56] 367 patients signed up
[4:02] 104 patients had embryo biopsy done
[4:38] 60 patients completed embryo transfer
[4:42] 15 live births
[4:44] 8 miscarriages
[4:45] 8 ongoing pregnancies
My thoughts:
The news about PGS trial was released in the press back in Nov 2016. At that time, I fulfilled two eligibility criteria and was qualified. Back then, it was before I had my 2nd miscarriage and before I had karyotyping done on my pregnancy tissues. Therefore, I was not aware of my actual problem. Before embarking on my 2nd fresh cycle, I asked my IVF doctor if I could be enrolled for PGS trial. However, at that time, there was a delay in the commencement of the trial and hence this was not an option for me if I didn't want to wait. By the way, PGS can only be done during a fresh cycle (at least in Singapore's SOP).
On hindsight, it was a blessing in disguise. Based on the karyotyping done in Oct 2017, my implantation failures and miscarriages were not likely due to chromosomal abnormalities. Also, based on the result of my recurrent pregnancy loss investigation, these were more likely due to thrombophilia aka sticky blood. Cost wise, it was way cheaper to do karyotyping (about $600) compared to PGS (about $3000) to find out that my embryos were normal. Ultimately, PGS would not have changed any outcome for me.
Looking at the statistics provided by MOH, at best 23 live birth out of 60 embryo transfer (38.3% success rate), doesn't seem very worth the investment. But to a couple wanting their own kid, all these numbers may not matter at all. I would try everything that somewhat make sense, until I have exhausted all options within my means.
One question that is significant to me - of these 15 lives births, how many had recurrent failed IVF or miscarriages? If these 15 patients are only 35 years and above, and not had failed IVF or miscarriages, it could be very possible that they would be successful without PGS. Considering the high out-of-pocket cost involved, I would think that they are more than just "35 years old and above".
I strongly believe that there needs to be more investigation before attempting PGS. But because there are so many unknowns and so many under-researched areas or research with conflictling/ inconclusive results, many OBGYN and IVF doctors remains doubtful of autoimmunity issues (perhaps with the exception of thyroid). But guess what, the controversial protocol worked for me!
$1.7 million of tax payer's money can be used in so many other ways to help the vulnerable groups and the under-privileged. I don't mean throwing out PGS all together because this may just be the answer, if there is no other explanation for the infertility after a truely thorough investigation including autoimmunity, sperm DNA fragmentation test, etc. And yes, my personal opinion is that the investigation at public hospitals are not thorough enough.
Monday, 1 March 2021
Trying for Mini J #2
| pre-cycle | Start 100mg aspirin* + 2mg (2 tabs) methyl folate* + 1000iu vitamin D* |
| CD2 | Start 8mg (4 tabs) progynova |
| CD5 | Start 10mg (2 tabs) prednisolone* |
| CD12 | Scan - lining 8.2mm trilaminar |
| CD14 | Start crinone twice daily + 0.4ml clexane* nightly |
| CD19 | ET at 2pm. Increase to 20mg (4 tabs) prednisolone* |
| 14dp5dt | beta-hCG - 1731.7 IU/L Received 1 shot of proluton^ + Start 10mg duphaston^ twice daily |
| 15dp5dt | Minor bleeding in the late evening. Increase to 20mg (2 tabs) duphaston twice daily. Stop clexane and aspirin |
| 18dp5dt | Received 1 shot of proluton |
| 19dp5dt | Spotting reduced. Restart clexane |
| 22dp5dt | Spotting stopped. Reduced to 10mg duphaston twice daily. |
| 31dp5dt | First fetal scan. No sac found. Chemical pregnancy. |
*Prescribed by Dr Sheila Vasoo
^Prescribed by Dr Marianne Hendricks
This round, perhaps due to COVID-19, KKIVF was rather empty every time I visited, a vast contrast to the crowd and long wait in the past. The pharmacy, however, was still as crowded as ever.
I was totally caught by surprise that I wouldn't be issued an MC on the day I have to return to KKH for beta-hCG blood test (which is compulsory by the way). Reason? Because I didn't see a doctor. It seems that this is not unique to KKH, NUH doesn't issue MC for the same reason. Didn't need the MC in my last cycle because I took no-pay leave. But I don't know why I only realise this in my 9th cycle; I can't recall if I ever asked for MC in my earlier cycles. If BFP, you have to go back in the afternoon to collect the papers for the next appointment and collect the medications, which meant another 2 hours spent at KKH. Anyway, no biggie for me, but I imagine some may get caught in a stressful situation.
I thought I should explain here that KKH typically prescribe duphaston after beta-hCG if BFP, but for me, Dr Sadhana agreed to my request to continue crinone but this also meant that duphaston wouldn't be in my protocol. Based on my previous pregnancy experience, I went to Dr Marianne Hendricks to ask for more support medications, in hope to prevent bleeding. But this time, bleeding started much earlier at week 4+ than my previous pregnancies (week 5+).
The first pre-natal scan (or dating scan) is typically scheduled 2 weeks after beta-hCG BT. I decided not to waste anymore time at KKH and went straight to my private doctor. At KKH, you have to see the sonographer for scan, then see the doctor to tell you the scan result and issue prescription, and finally queue at the pharmacy to buy medicine. This is too much waiting time for me.
What's the biggest difference between my previous pregnancy and this one? Back in 2018, I had very bad nausea, indigestion and tiredness, starting from around week 5, but all these symptoms have yet to surface at week 6. I was right to be paranoid and worried. How can I be so lucky not to have any major morning sickness this time round. Indeed, something went wrong.
At week 7 (or maybe almost week 7), there was no sac. It was a chemical pregnancy.

Goodbye my angel baby...
Monday, 8 February 2021
Gift from God

(Click on image to go to website.)
A timely reminder that J is "given to us... as an assignment" and we are "to be stewards, responsible to love him, nurture him and bring him up..."
Considering how difficult it was for us to have J, I always have an irrational fear that something bad would happen or I would lose J one day. I need to find peace, let go and let God.
Friday, 8 January 2021
Filling in the Gap
What happened in 2018? It was a year of many changes. Most importantly, it was the year my rainbow baby was born.
After my 2nd miscarriage Oct 2017 and knowing that my angel baby is chromosomally normal, I went for a blood test to check my progesterone level during luteal phase and did a sonohysterography as suggested by Dr Sadhana. Conclusion, progesterone level wasn't ideal to try natural FET (with ovulation medication), while sonohysterography result came back normal.
In Apr 2018, I embark on yet another medicated frozen cycle. By then, I have exhausted the 15k Medisave limit and this cycle was fully pay by cash. In May 2018, my beta-hCG was at 1893 IU/L, much higher than frozen #5, but it wasn't time to celebrate yet. True enough, I started bleeding at around week 5, just like previous miscarriages. For the sake of familiarity, I went to KKH 24-hour O&G, and it turned out to be a complete waste of time. Out of desperation, I asked for an urgent appointment to see Dr Sheila Vasoo, who referred me to Dr S F Loh and I saw him on the same day. I was given a proluton jab and my bleeding stopped. However, the bleeding started again about 1 week later and Dr Loh gave me another jab. It happened again at week 8 and thankfully, that was the last episode. The following months went on peacefully, except for the very bad morning sickness that finally went away in 2nd trimester, and the very bad itchy rashes in 3rd trimester.
What was different between frozen #6 and the earlier ETs?
I wouldn't know if it was the higher progesterone support or the higher doses of clexane and prednisolone (or both) that helped. Most O&G doctors view that all these are not neccessary; they don't believe in Dr Sheila's protocol. "Duphaston is sufficient" they said. "You don't need the blood thinners and prednisolone" they said. They are right, based on scientific evidences which probably wrote that 95% of the candidate showed positive outcome with duphaston twice daily. But they could be wrong, for the minority who do not fall within the statistic.

Day 2 embryos x6, Day 5 blastocysts x3, Clexane jabs x276 (from 0.2 ml to 0.4 ml to 0.5 ml).
After my 2nd miscarriage Oct 2017 and knowing that my angel baby is chromosomally normal, I went for a blood test to check my progesterone level during luteal phase and did a sonohysterography as suggested by Dr Sadhana. Conclusion, progesterone level wasn't ideal to try natural FET (with ovulation medication), while sonohysterography result came back normal.
In Apr 2018, I embark on yet another medicated frozen cycle. By then, I have exhausted the 15k Medisave limit and this cycle was fully pay by cash. In May 2018, my beta-hCG was at 1893 IU/L, much higher than frozen #5, but it wasn't time to celebrate yet. True enough, I started bleeding at around week 5, just like previous miscarriages. For the sake of familiarity, I went to KKH 24-hour O&G, and it turned out to be a complete waste of time. Out of desperation, I asked for an urgent appointment to see Dr Sheila Vasoo, who referred me to Dr S F Loh and I saw him on the same day. I was given a proluton jab and my bleeding stopped. However, the bleeding started again about 1 week later and Dr Loh gave me another jab. It happened again at week 8 and thankfully, that was the last episode. The following months went on peacefully, except for the very bad morning sickness that finally went away in 2nd trimester, and the very bad itchy rashes in 3rd trimester.
What was different between frozen #6 and the earlier ETs?
| FET#1 to FET#4 | FET#5 | FET#6 | |
| Progynova | ✔ | ✔ | ✔ |
| Crinone (pre beta-hCG BT) | ✔ | ✔ | ✔ |
| Crinone (post beta-hCG BT) | ✔ | ||
| Duphaston | ✔ | ✔ | ✔ |
| Proluton | weekly from week 6 to 8 | ||
| Aspirin | ✔ | ✔ | |
| Clexane | 0.2 ml | 0.4 ml | |
| Prednisolone | 10 mg | 20 mg | |
| Folic Acid | ✔ | ✔ | |
| Folate | ✔ | ||
| Vitamin D | ✔ | ✔ |
I wouldn't know if it was the higher progesterone support or the higher doses of clexane and prednisolone (or both) that helped. Most O&G doctors view that all these are not neccessary; they don't believe in Dr Sheila's protocol. "Duphaston is sufficient" they said. "You don't need the blood thinners and prednisolone" they said. They are right, based on scientific evidences which probably wrote that 95% of the candidate showed positive outcome with duphaston twice daily. But they could be wrong, for the minority who do not fall within the statistic.
Day 2 embryos x6, Day 5 blastocysts x3, Clexane jabs x276 (from 0.2 ml to 0.4 ml to 0.5 ml).
Wednesday, 6 January 2021
Government Support for IVF

(Click on image to go to CNA website.)
Summary of Mr Louis Ng's proposals:
| 1. | Increase number of subsidised IVF cycles from 6 to 8 [2:53] |
| 2. | Introduce subsidy for PGD and allow balance to paid out of Medisave (subjected to a limit) [5:13] |
| 3. | Remove quota on number of fresh and frozen cycles for subsidised IVF treatment [7:19] |
| 4. | Introduce "fertility leave" for both husband and wife [8:30] |
My thoughts:
Firstly, I deeply appreciate Mr Louis Ng's consistent and persistent push for the government to provide better support for couples undergoing fertility treatment. It is through him that our difficulties can be heard at a wider platform. Unfortunately, this year really isn't a good year to expect the government to put in more budget for this; we are already in budget deficit due the covid-19. And of course, from the government's perspective, the more cost-effective way to sustain or improve birth rate is by dishing out more baby bonus (effective or not, is a debate for another day). I believe Mr Louis Ng knows that the chance is slim for his proposals to be adopted this year, nonetheless, it is a topic important enough to be tabled in Parliament.
It is interesting to note that there is flexibility to request for government co-funding beyond the 3rd fresh or frozen cycles, if the couple have used co-funding for less than 6 cycles, but 4th and 5th fresh cycle co-funding limit follows frozen cycle at $2,200 [23:36]. In my case, after I have used up co-funding for 2 fresh and 3 frozen cycles (and 3 frozen without co-funding), I can request for my next frozen cycle to be co-funded (as I still have 1 blastie in the freezer now). However, there is no granted success, I think it is safer to reserve my very last co-funding for a 3rd fresh cycle, which is a lot more expensive than frozen cycle, just in case frozen #7 turns out to be BFN.
Personally, I feel that simply increasing the number of subsidised cycles might not help. I think the medical team needs to be more aggressive in the treatment. My 8th cycle was successful because I was on a whole lot of medications. No one likes to pop 10 pills or get injections everyday for months. But if this is necessary, many of us would be willing to do it just so that we can have children. If the hospital SOP encourages more tests to be done or provide more support medications after a failed cycle, I wouldn't have to go through as many as 3 BFN and 2 miscarriages, which not just waste the government co-funding and medisave funds, but also bring more disappointments. If I have not met Dr Sheila Vasoo and Dr S F Loh, I would not have my mini J today. (I have yet to share the details of my successful frozen #6 and perhaps it is time for me do so soon.)
After 8 IVF cycles, I have used up the $15k cap from Medisave. So, my wish is to allow me to tap on my excess Medisave funds. Every year, there would a decent amount being transferred from my Medisave to Special account, because there is a maximum balance for Medisave account (current is $60k). And so, my money is locked away in Special account, collecting interest and waiting for the day I retire. This is one logic that I cannot appreciate because the government already has measures in place to ensure a comfortable retirement.
I count myself lucky to have a secure and stable job, and luckier that I have an understanding boss. At the start of my 8th cycle, I applied for one year no-pay leave. When mini J was 4 months old, I returned to work. Whether "fertility leave" is useful or not, probably depends on one's circumstances. Applying for "fertility leave" outrightly reveals that you are going for fertility treatment, which still carrys a negative connotation and not everyone is ready to share at that point in time. Would it make the situation worst? Some people lose their jobs after returning from maternity leave. Would the company take the opportunity to axe the staff knowing that she is planning to have a child?
Subscribe to:
Posts (Atom)